Abstract
Background
Alcohol-related harm has been found to be higher in disadvantaged groups, despite similar alcohol consumption to advantaged groups. This is known as the alcohol harm paradox. Beverage type is reportedly socioeconomically patterned but has not been included in longitudinal studies investigating record-linked alcohol consumption and harm. We aimed to investigate whether and to what extent consumption by beverage type, BMI, smoking and other factors explain inequalities in alcohol-related harm.
Methods
11,038 respondents to the Welsh Health Survey answered questions on their health and lifestyle. Responses were record-linked to wholly attributable alcohol-related hospital admissions (ARHA) eight years before the survey month and until the end of 2016 within the Secure Anonymised Information Linkage (SAIL) Databank. We used survival analysis, specifically multi-level and multi-failure Cox mixed effects models, to calculate the hazard ratios of ARHA. In adjusted models we included the number of units consumed by beverage type and other factors, censoring for death or moving out of Wales.
Results
People living in more deprived areas had a higher risk of admission (HR 1.75; 95% CI 1.23–2.48) compared to less deprived. Adjustment for the number of units by type of alcohol consumed only reduced the risk of ARHA for more deprived areas by 4% (HR 1.72; 95% CI 1.21–2.44), whilst adding smoking and BMI reduced these inequalities by 35.7% (HR 1.48; 95% CI 1.01–2.17). These social patterns were similar for individual-level social class, employment, housing tenure and highest qualification. Inequalities were further reduced by including either health status (16.6%) or mental health condition (5%). Unit increases of spirits drunk were positively associated with increasing risk of ARHA (HR 1.06; 95% CI 1.01–1.12), higher than for other drink types.
Conclusions
Although consumption by beverage type was socioeconomically patterned, it did not help explain inequalities in alcohol-related harm. Smoking and BMI explained around a third of inequalities, but lower socioeconomic groups had a persistently higher risk of (multiple) ARHA. Comorbidities also explained a further proportion of inequalities and need further investigation, including the contribution of specific conditions. The increased harms from consumption of stronger alcoholic beverages may inform public health policy.
Background
Alcohol consumption is a leading risk factor for population health worldwide [1]. Measures of alcohol-related harm such as hospital admissions and mortality show particularly wide inequalities and reducing inequalities is a focus of governments [1,2,3,4]. Alcohol-related harm has been found to be higher in disadvantaged groups, despite comparable or even lower reported alcohol consumption than in advantaged groups [5, 6]. This phenomenon has been termed the ‘alcohol harm paradox’. A number of hypotheses to explain it have been suggested in the literature [5, 7,8,9].
The first hypothesis is that there may be different patterns of alcohol consumption across groups rather than simply unit consumption or whether a threshold of consumption is reached. Overall, average consumption may not differ between groups but if all alcohol is consumed in one sitting peak toxicity is greater in those who binge drink. More deprived groups are more likely to drink at extreme levels, potentially in part explaining the paradox [8]. The type of alcoholic beverage may also offer an explanation. Consumption of spirits or beer has been associated with worse “trouble per litre” than wine, and consumption of spirits have been associated with increased alcohol poisoning and aggressive behaviour [10, 11]. It has also been suggested that the poorest outcomes are found for beverages chosen by young men [10]. A potential mechanism could be the faster absorption of alcohol from stronger drinks or other characteristics of the people with a particular beverage preference, but the reasons for differing outcomes by beverage type are not well understood.
The second hypothesis concerns the combination of challenging health behaviours or comorbidities typically found in more disadvantaged groups. This combination causes proportionately poorer outcomes compared to similar alcohol consumption in advantaged groups. Deprived higher risk drinkers were found to be more likely to drink alcohol combined with other “health-challenging behaviours that include smoking, being overweight, poor diet and lack of exercise” compared to more affluent groups [7]. There are also known associations between mental health and alcohol consumption which could affect disadvantaged groups differently [12].
The third hypothesis relates to underestimating consumption in disadvantaged groups and the alcohol harm paradox not existing or being an artificial construct. Response bias may be at work where those who do not respond to the survey could have systematically different consumption levels or worse outcomes compared to responders [13]. Moreover, current drinking may not reflect the life history of harmful drinking, which has been found to be associated with deprivation in lower and increased risk drinkers [7].
A few recent cross-sectional studies have investigated the harm paradox, but mostly considered drinking patterns and their influence on the paradox rather than outcomes of harm [7, 8]. Only one longitudinal study in Scotland has employed record-linkage between consumption patterns and harm, investigating socioeconomic status as an effect modifier, but did not include the type of beverage or multiple admissions [5].
This study aims to investigate whether and to what extent individual alcohol consumption by type of beverage, smoking, BMI and other factors could account for inequalities in alcohol-related hospital admission (ARHA). A different risk of harm by socioeconomic group for a given level of individual consumption could be an explanation of the alcohol-harm paradox at group level. Additionally, we examine how the patterns of consumption by type of beverage differ by socioeconomic group.
Methods
Data
This analysis was carried out using the Electronic Longitudinal Alcohol Study in Communities (ELAStiC) data platform and details on the data and linkage methods are outlined in the study protocol [14]. A summary and further specific details for this study are described below.
Welsh health survey
Our cohort consisted of 11,038 people aged 16 and over who responded to the Welsh Health Survey in 2013 and 2014, consenting to have their survey responses linked to routine health data. The Welsh Health Survey is an annual population survey on health and health-related lifestyle based on a representative sample of people living in private households in Wales (random sampling). It consists of a short interview with the head of household and a self-completed questionnaire for each individual adult aged 16 years and above in the household. A question on consent for data linkage was included from April 2013 to December 2014 and approximately half of the respondents agreed. Originally 11,694 respondents agreed to their data being linked, and records were successfully linked and anonymised into the SAIL Databank through standard split file processes for 11,320 individuals (3.2% loss) [14]. Linkage to records of household residence needed for analysis failed for 282 respondents, resulting in the final sample of 11,038 people (5.6% loss overall). An overview of characteristics of the study population is shown in Table 1.
Table 1 Characteristics of the study population
| Men | Women | Total | |
|---|---|---|---|
| Survey year | |||
| 2013 | 1906 (37%) | 2269 (38%) | 4175 |
| 2014 | 3199 (63%) | 3664 (62%) | 6863 |
| Age group | |||
| 16–29 years | 716 (14%) | 998 (17%) | 1714 |
| 30–44 years | 914 (18%) | 1202 (20%) | 2116 |
| 45–59 years | 1277 (25%) | 1522 (26%) | 2799 |
| 60–74 years | 1518 (30%) | 1502 (25%) | 3020 |
| 75+ years | 680 (13%) | 709 (12%) | 1389 |
| Area deprivation | |||
| More deprived 40% | 1826 (36%) | 2170 (37%) | 3996 |
| Less deprived 60% | 3279 (64%) | 3763 (63%) | 7042 |
| Alcohol consumption* | |||
| None | 526 (10%) | 854 (13%) | 1380 |
| Not binge | 3041 (64%) | 3740 (69%) | 6783 |
| Binge | 1440 (26%) | 1197 (18%) | 2637 |
| Mean units (drinkers only) | |||
| Beer or Cider | 6.3 (6.7) | 1.6 (3.7) | 4.0 (6.1) |
| Wine or Champagne | 2.1 (4.1) | 3.8 (4.7) | 2.9 (4.5) |
| Spirits or other | 1 (2.7) | 1.5 (3.1) | 1.2 (2.9) |
| Any type | 9.5 (7.8) | 6.9 (5.8) | 8.2 (7.0) |
| Smoking status* | |||
| Never smoker | 2242 (44%) | 3073 (52%) | 5315 |
| Ex-smoker | 1837 (36%) | 1670 (28%) | 3507 |
| Smoker | 972 (19%) | 1136 (19%) | 2108 |
| Mean BMI (SD) | 27.2 (4.84) | 27 (5.94) | 27.1 (5.4) |
| Total person-years | 29,221.1 | 34,417.8 | 63,638.9 |
| Number of admissions | 169 | 110 | 279 |
- Number of respondents (%) or mean units (Standard deviation, SD)
- *Numbers do not sum due to missing data
Measures of socioeconomic status
We used an area-based deprivation measure (i), the Welsh Index of Multiple Deprivation (WIMD) 2011 [15], as well as four individual-level measures of socioeconomic status from survey responses (ii) social class, iii) employment, iv) housing tenure, and v) highest qualification). We linked the WIMD to each Lower layer Super Output Area (LSOA) of residence at survey month. We grouped the two more deprived quintiles and three less deprived quintiles because of relatively small numbers.
Alcohol consumption
Respondents were also asked about the frequency of drinking, including whether or not they had drunk alcohol at all during the past year and the number of each type of alcoholic beverage they had consumed on the heaviest drinking day in the past week. These include categories of, for example, “small can of strong beer”, “small glass of wine”, as well as free text for additional drinks not listed. These data were converted into units (8 g ethanol per unit) consumed by beverage type, and capped at 60 units to deal with a very small number of responses of between 60 and 120 units, likely a misreading of units. We created three groups: 1) beer and cider; 2) wine and champagne; 3) spirits, alcopops, fortified wine and others. There were relatively small numbers of alcopops, fortified wine and others and so we combined these with the spirits. Our sensitivity analysis showed that the inclusion of these drinks did not alter the results for this category which was predominantly made up of spirits.
Outcome measure of alcohol-related hospital admission
The outcome was (multiple) alcohol-related hospital admission(s). We selected the earliest episode in each hospital spell with a wholly attributable diagnosis included in the definition outlined in the study protocol [14]. These are similar to the alcohol-specific definition used by Public Health England with a few additional codes [14, 16]. These could be the primary diagnosis or a secondary diagnosis in any position. This included multiple admissions for survey respondents. The details of the data source, linkage and extraction are outlined in the study protocol [14].
Other survey measures
Other measures used based on survey responses were smoking, BMI, general health and being treated for a mental health condition. Smoking was coded into three categories: 1) regular or current smoker, 2) Ex-smoker and 3) never smoker. BMI was readily calculated based on self-reported height and weight. Respondents were asked about their general health which we coded into the following two groups: 1) Poor and fair health, 2) good, very good and excellent health. Respondents were also asked whether they were currently being treated for depression, anxiety or another mental illness (yes/no). This was coded into a binary variable with values of being treated for any mental health condition listed or not treated if none was selected.
Study design/processing
Survey responses were record-linked within the SAIL Databank to hospital admission data (Patient Episode Database for Wales), mortality data (Annual District Death Extract from the Office for National Statistics) and data containing residence and thus house moves (Welsh Demographic Service Dataset) as outlined in the study protocol [14]. All data was extracted for eight years before the survey month until the end of the year 2016. The study period ran from three years before the survey in 2013 or 2014 to the end of 2016, with a study period of between five and six years depending on when the survey was undertaken. We structured the data so that each person could contribute multiple time periods, if they had an admission, with the number of admissions up to the current time period counted during the study. We also considered the number of historic alcohol-related admissions during the five years before study start (i.e. 8 years before to 3 years before the survey date, or 2005–06 to 2010–11) as a covariate in the modelling analysis. We censored for death or moving out of the study area (Wales). An illustration of the study timeline is shown in Fig. 1. We also performed a sensitivity analysis using the data restricted to time periods after the survey date only (2013/14 to the end of 2016) for comparison.
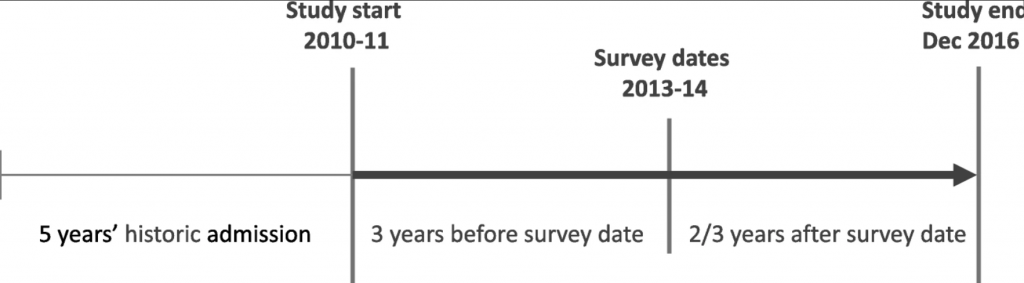
Figure 1 : Illustration of study timeline
Statistical analyses
We estimated hazard ratios (HR) with 95% confidence intervals (95% CIs) for the risk of (multiple) alcohol-related hospital admission associated with each socioeconomic group using multi-level Cox mixed effects models [17]. We used a recurrent event model with admission as the outcome and using age as the underlying timescale rather than calendar time. We used Cox proportional hazards models stratified by the current count of admission events to date (during the study period), so that each unique admission count has a separate baseline hazard function. Including admission counts during the study period as strata accounts for covariance within an individual’s recurrent events and is similar to a frailty model [18]. Details of covariates in each model are given below, but in every case their hazard ratios were assumed constant across strata. Additionally, a random effect at the household level was used in the multilevel analysis to allow for potential similarities in responses within a household over and above their individual characteristics. All analyses were conducted using R [20], specifically using the coxme function [21]. To deal with missing observations for BMI, unit consumption, smoking and individual-level socioeconomic measure we used 20 iterations of multiple imputation using chained equations using the package MICE in R [19]. This was chosen for efficiency to avoid reducing the sample size.
The number of historic events during the 5 years before study start was included as a covariate in all models. This was chosen to account for differences in risk of the next admission, because people with a prior admission were more likely to have another admission than those who did not.
The first basic model (Model A) adjusted for area deprivation, sex and the number of historic ARHA during 5 years before study start. Model B additionally adjusted for the number of units reported by drink type (beer and cider; wine and champagne; spirits including alcopops) on the heaviest drinking day in the past week, smoking status and BMI. We repeated the basic and adjusted model using area deprivation (i) for all other individual measures of socioeconomic status, ii) social class, iii) employment, iv) housing tenure, and v) highest qualification, to compare estimates in the basic model with those of the adjusted model. We also included an interaction term in adjusted Model B between BMI and total unit consumption.
Model C, also based on the adjusted model B, additionally included self-reported general health, and Model D added self-reported treatment for a mental health condition to investigate comorbidities.
Two additional models were used to investigate the contribution of the units for each specific beverage type to inequalities. These were based on Model A, but also included the total units consumed and, separately, the units for each type of drink as covariates (results not shown). Another model included the frequency of drinking (results not shown).
For the sensitivity analysis we have re-run all models above on the limited dataset including only the time periods following the survey date. The results were compared to the main results using the extended dataset.
Finally, we also analysed the mean units of alcohol consumed by beverage type and by age, sex and deprivation group, including 95% confidence intervals (Fig. 2). To show the distribution of units in each group we have also included boxplots for any type of beverage with the outliers removed due to data non-disclosure rules associated with the record-linked environment.
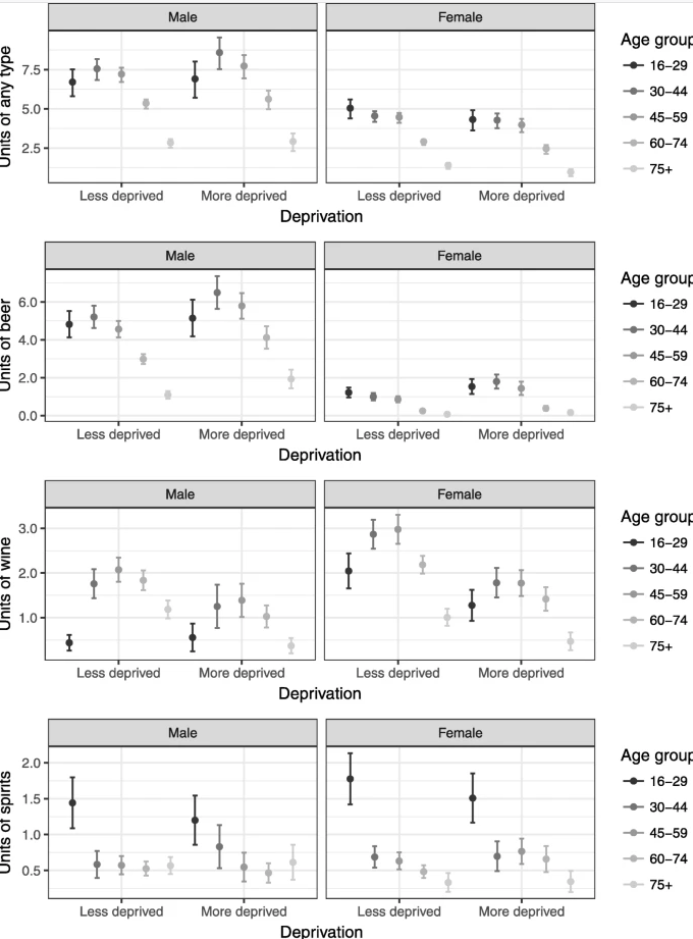
Figure 2 : Mean units for by beverage type, age, sex and deprivation group (including 95% confidence intervals)
Results
Sample characteristics
Our study sample consisted of 11,038 respondents with a total of 63,638.9 person-years of follow-up. There were 279 alcohol-related admissions during the study period (131 individuals with one or more admission). The crude rate per 1000 person-years was 4.38. An overview of our sample characteristics is shown in Table 1 . There were more females than males. Key demographic data was complete in the survey but there were missing responses to some of the individual survey questions, ranging from 0.6% for drinking frequency to 4.9% for BMI. Modelling analyses use imputation to deal with missing responses, but Table 1 shows completed and valid responses only and therefore the sums for each characteristic may be different, for example between sums for alcohol consumption and smoking status.
Patterns of consumption
Deprived groups had larger proportions of people who reported not drinking at all in the past year (15% compared to 11%, Table 2), and also higher proportions who did not drink in the past week but reported some drinking in the past year (47% compared to 37%, Table 2). However, those who drank in the deprived group had slightly higher proportions of people who binged (more than 4 units for men and more than 3 units for women) on a single occasion, with 25.8% in the deprived group compared to 23.6% in the less deprived group. This suggests that fewer people drank in deprived groups but, those who had any alcohol, drank more. Some of those who either did not drink at all in the past year, or reported some drinking in the past year but no units in the past week had an alcohol-related admission at some point during the study period. This could suggest that ongoing health concerns might explain their abstinence [22].
Table 2 Alcohol consumption by deprivation group and whether admitted
| Less deprived | More deprived | |||
|---|---|---|---|---|
| N (%) | with admission | N (%) | with admission | |
| Drinking frequency* | ||||
| Not at all in the past year | 785 (11.2) | 8 | 595 (15.0) | 7 |
| Less than weekly | 2404 (34.3) | 9 | 1575 (39.7) | 19 |
| More than weekly | 3813 (54.5) | 43 | 1802 (45.4) | 45 |
| Binge drinking* | ||||
| None in past week | 2573 (37.3) | 17 | 1834 (46.9) | 28 |
| Some but not binge | 2688 (39.0) | 19 | 1068 (27.3) | 16 |
| Binge | 1628 (23.6) | 22 | 1009 (25.8) | 27 |
| Drank at least one unit of* | ||||
| Beer or Cider | 2121 (30.8) | 27 | 1269 (32.4) | 31 |
| Wine or Champagne | 2336 (33.9) | 16 | 759 (19.4) | 13 |
| Spirits or other | 1242 (18.0) | 14 | 656 (16.8) | 16 |
| Total cohort | 7042 | 60 | 3996 | 71 |
Overall, the mean units of total alcohol consumed were similar or slightly higher in the more deprived group than the less deprived group for males but similar or slightly lower for females (Fig. 2). If only those who drank are compared (chart not shown) then men in the more deprived group drank more on average than men in the less deprived group for all age groups with smaller differences in women.
Socioeconomic patterns differed by type of beverage. Similar to any type, mean units of beer were slightly higher in more deprived groups, and unit consumption much higher for men than women. The pattern for wine was the opposite showing lower consumption in more deprived, with the exception of the youngest men. More spirits were consumed by younger drinkers with only slightly lower averages for the deprived group. There was little difference in the more deprived group in most other age groups of those aged 30 and above compared to less deprived groups. The box plots in Fig. 3 for units of any type of beverage show that the distribution is skewed towards lower reported units reflecting the large proportion of people reporting zero units, particularly in the youngest and oldest age groups. The medians for younger males in more deprived groups are lower than the less deprived, and for females the medians are lower in the more deprived for most age groups.
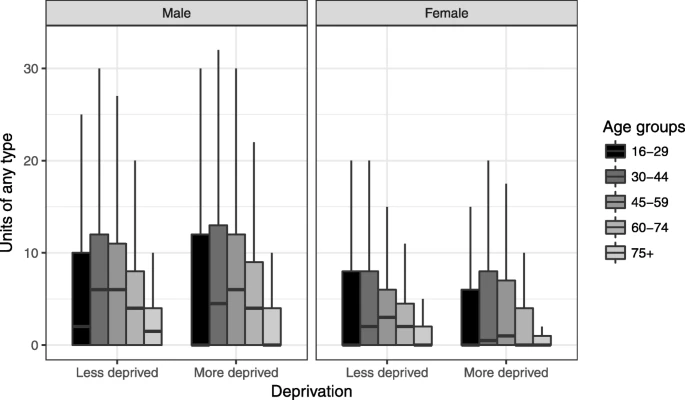
Figure 3 : Box plot for any type of beverage by age group, sex and deprivation group (outliers removed)
Factors associated with alcohol-related hospital admission
A total of 131 out of 11,038 respondents had at least one ARHA during the study period. Women tended to have a lower risk of admission than men (HR 0.71; 95% CI 0.51–0.99, Model A in Table 3), although this was only statistically significant in Model A, and not in the fully adjusted Model B. Smoking had the strongest association with alcohol-related hospital admission and smokers were 4.53 times more likely to have an admission (HR 4.53; 95% CI 2. 85–7.21, Model B) than those who were never smokers. Ex-smokers were 1.50 times more likely to have an admission compared to the same reference group, although this was not statistically significant. BMI appeared to be slightly protective, but it was not statistically significant (HR 0.98; 95% CI 0.94–1.01, Model B). We also investigated the interaction between BMI and total unit consumption based on Model B but we found no evidence for an interaction (results not shown).
Table 3 Results of regression models using area deprivation: hazard ratios for the risk of alcohol-related hospital admission for each model covariate
| Basic model (Model A) | Adjusted model (Model B), adjusted for units, smoking and BMI | |
|---|---|---|
| HR (95% CI; p-value) | HR (95% CI; p-value) | |
| Men (ref) | 1 | 1 |
| Women | 0.71 (0.51–0.99; 0.046) | 0.72 (0.50–1.06; 0.095) |
| Less deprived 60% (ref) | 1 | 1 |
| More deprived 40% | 1.75 (1.23–2.48; 0.002) | 1.48 (1.01–2.17; 0.043) |
| Number of historic adm. | 1.38 (1.28–1.49; < 0.001) | 1.38 (1.26–1.52; < 0.001) |
| Units beer and cider | 1.02 (0.99–1.05; 0.137) | |
| Units wine and champagne | 1.03 (0.99–1.07; 0.127) | |
| Units spirits and other | 1.06 (1.01–1.12; 0.016) | |
| Never smoker (ref) | 1 | |
| Ex-smoker | 1.50 (0.90–2.49; 0.119) | |
| Smoking | 4.53 (2.85–7.21; < 0.001) | |
| BMI | 0.98 (0.94–1.01; 0.224) |
Table 4 Comparison of regression model results: hazard ratios for the risk of alcohol-related hospital admission for each socioeconomic measure
| Events | Person-years | Basic model | Adjusted model | |
|---|---|---|---|---|
| HR (95% CI; p-value) | HR (95% CI; p-value) | |||
| i) Area deprivation (Model A/B) | ||||
| Less deprived 60% (ref) | 148 | 39,801.1 | 1 | 1 |
| Most deprived 40% | 131 | 23,837.7 | 1.75 (1.23–2.48; 0.002) | 1.48 (1.01–2.17; 0.043) |
| ii) Social class (NSSEC) | ||||
| Professional and managerial (ref) | 80 | 25,623.1 | 1 | 1 |
| Intermediate | 39 | 11,277.2 | 1.52 (0.86–2.7; 0.152) | 1.3 (0.67–2.52; 0.436) |
| Routine and manual | 146 | 25,297.1 | 2.03 (1.3–3.15; 0.002) | 1.81 (1.09–3; 0.022) |
| Never worked/long-term unempl. | 14 | 1441.5 | 5.65 (2.49–12.82; < 0.001) | 4.04 (1.55–10.51; 0.004) |
| iii) Employment | ||||
| Employed (ref) | 36 | 30,724.8 | 1 | 1 |
| Not employed | 243 | 32,914.1 | 3.87 (2.24–6.69; < 0.001) | 3.38 (1.97–5.65; < 0.001) |
| iv) Housing Tenure | ||||
| Home owner (ref) | 127 | 47,376.9 | 1 | 1 |
| Private rental | 15 | 7104.5 | 1.13 (0.56–2.27; 0.729) | 1 (0.49–2.07; 0.992) |
| Social rental | 137 | 9154.4 | 3.97 (2.73–5.77; < 0.001) | 2.89 (1.9–4.42; < 0.001) |
| v) Highest qualification | ||||
| Degree (ref) | 66 | 11,254.9 | 1 | 1 |
| Other | 117 | 39,486.6 | 1.25 (0.72–2.15; 0.428) | 1.03 (0.57–1.84; 0.926) |
| None | 96 | 12,897.4 | 2.38 (1.32–4.31; 0.004) | 1.78 (0.93–3.4; 0.083) |
Adjusting for the total number of units regardless of type of beverage (results not shown) gave very similar results to Model B with an elevated risk of ARHA in the most deprived group (HR 1.46; 95% CI 1. 01–2.11). This suggests that the type of beverage was not important over and above the number of units relating to inequalities.
For models C and D the risk of ARHA in the more deprived group was reduced further compared to Model B (Poor health by 16.6%: HR 1.36; 95% CI 0.92–2.00; being treated for mental health condition by 5.0%: HR 1.45; 95% CI 0.96–2.17, Table 5). This risk in disadvantaged groups, although still elevated, was not statistically significant. Although this will need further research relating to interactions and specific conditions, it suggests that comorbidities, either relating to alcohol or otherwise, could be important.
Table 5 Results of regression models for area deprivation investigating comorbidities: hazard ratios for the risk of alcohol-related hospital admission for each model covariate
| Adjusted model, including general health (Model C) | Adjusted model including treated for mental health condition (Model D) | |
|---|---|---|
| HR (95% CI; p-value) | HR (95% CI; p-value) | |
| Men (ref) | 1 | 1 |
| Women | 0.71 (0.47–1.06; 0.092) | 0.63 (0.42–0.95; 0.026) |
| Less deprived 60% (ref) | 1 | 1 |
| More deprived 40% | 1.36 (0.92–2.00; 0.120) | 1.45 (0.96–2.17; 0.074) |
| Number of historic adm. | 1.35 (1.22–1.48; < 0.001) | 1.35 (1.23–1.47; < 0.001) |
| Units beer and cider | 1.03 (1–1.05; 0.052) | 1.02 (0.99–1.04; 0.197) |
| Units wine and champagne | 1.03 (1–1.07; 0.068) | 1.03 (0.98–1.07; 0.239) |
| Units spirits and other | 1.07 (1.02–1.13; 0.009) | 1.06 (1.01–1.12; 0.025) |
| Never smoker (ref) | 1 | 1 |
| Ex-smoker | 1.38 (0.83–2.32; 0.216) | 1.48 (0.88–2.51; 0.141) |
| Smoker | 4.10 (2.56–6.56; < 0.001) | 3.88 (2.37–6.35; < 0.001) |
| BMI | 0.97 (0.93–1.01; 0.101) | 0.98 (0.94–1.02; 0.257) |
| Good health (ref) | 1 | |
| Poor health | 2.89 (1.91–4.37; < 0.001) | |
| Not treated for mental health condition (ref) | 1 | |
| Treated for mental health condition | 2.66 (1.72–4.11; < 0.001) |